
Quality measurement: Making it meaningful
America’s hospitals are committed to sharing meaningful, accurate hospital quality information with the patients they serve. Hospitals also support well-designed pay-for-performance programs that can help move the health care delivery system from volume to value.
At the same time, however, hospitals, their clinicians and the post-acute care organizations they work with are asked to provide data on a dizzying array of quality measures. The burden of collecting many of these measures often outweighs the benefit, and consumers can be confused by the volume of information.
Measure collection and reporting would advance progress on important quality issues more quickly and effectively if federal agencies and others asking for data agreed on a manageable list of high-priority aspects of care — providers could be asked to make meaningful improvement in these areas. Then, a small and critically important set of measures could be used to track and report on progress toward improving care delivered and outcomes for patients.
The American Hospital Association is working with federal health officials to streamline and prioritize quality measurement efforts. To make meaningful progress, it is critical that Medicare and other federal programs better align and prioritize measurement efforts to address the most important issues and promote more patient-centered, effective and efficient care.
History report
More than a decade ago, hospitals initiated voluntary efforts to report quality data to the public. This data reporting was later linked to receiving a full annual payment update from Medicare through the Hospital Inpatient Quality Reporting and Hospital Outpatient Quality Reporting programs.
The Affordable Care Act significantly raised the financial stakes of quality measurement by introducing pay-for-performance programs — including the Hospital Value-Based Purchasing Program, Hospital Readmissions Reduction Program and Hospital-Acquired Condition Reduction Program — that tie a portion of hospitals’ Medicare reimbursement to their performance on certain quality measures. To date, however, HRRP penalties have disproportionately fallen on those hospitals caring for the poorest patients. Moreover, the HACRP disproportionately penalizes large and teaching hospitals caring for patients with complex conditions, and the smallest hospitals with too few patients for accurate assessment.
Hospitals and health systems continue to believe that quality measurement and pay for performance must align with the health care field’s movement from volume to value. There are significant concerns, however, that the explosion in measure-reporting requirements is limiting the effectiveness of efforts to improve quality and causing confusion for the public. The fact that hospitals will have a total of 94 measures in Centers for Medicare & Medicaid Services hospital quality reporting and pay-for-performance programs in 2019 underscores the need to further streamline measures. Further, many of the measures chosen by CMS are not related to issues that meaningfully improve care for patients. As a result, they increase the burden of collecting data without adding value to care. Compounding the dilemma, private payers and other regulatory bodies require the reporting of yet additional measures.
Many hospital leaders and clinicians also are frustrated by the multitude of hospital pay-for-performance programs and report cards, each of which uses different measures and methodologies for rating performance. Most recently, CMS introduced “star ratings” for acute care hospitals on its Hospital Compare website. These ratings, like those for movies or restaurants, give hospitals one to five stars based on performance on a select subset of measures.
The star ratings, though, raise far more questions than they provide answers and add to a long list of conflicting rating and ranking systems. Hospitals are especially troubled that the current rating scheme used by CMS unfairly penalizes teaching hospitals and those serving disproportionately higher numbers of the poor. As constructed, the system falls short of meeting principles that the AHA has embraced for quality report cards and rating systems.
AHA efforts
The AHA has pursued a number of strategies to streamline measure data reporting requirements and to focus programs on “measures that matter.”
Identifying hospital measure priorities: In 2013 and 2014, the association’s governance committees discussed and prioritized measurement topics for use in assessing and incentivizing hospitals and health care systems. The AHA board of trustees then approved a list of 11 hospital quality performance priority topics. In response to subsequent feedback from regional policy boards along with council and committee discussions on quality measures, the AHA board in July adopted minor updates to the list of priority measure topics:
- Patient safety outcomes (harm rates, infection rates, medication errors).
- Readmission rates.
- Risk-adjusted mortality.
- Effective patient transitions.
- Diabetes control.
- Obesity.
- Adherence to guidelines for commonly overused procedures.
- End-of-life care according to preferences.
- Cost per case or episode of care.
- Behavioral health (added July 2016).
- Patient experience of care/patient-reported outcomes of care.
In addition, in 2015, the AHA board voted to endorse the Institute of Medicine’s Vital Signs recommendations and urged other national public and private entities to also approve these recommendations to align and streamline national health improvement efforts around a common set of focus areas and measures. Vital Signs is a unifying framework that identifies 15 core measurement priorities common to all stakeholders in health: providers, public and private payers, public health agencies, and patients. These 15 areas dovetail well with the AHA’s list of 11 hospital performance priorities.
The AHA continually uses the AHA priority measures and Vital Signs report in advocacy efforts with CMS, the National Quality Forum and others.
Strategic principles
To better focus the debate over quality measures and ensure that national quality goals are being advanced through measurement, the AHA believes it is important to develop a set of strategic principles that establish the parameters for “measures that matter.” As such, the AHA supports the following principles for measures to be used in public reporting and incentive programs:
- Provider behavior must influence the outcome being measured.
- There must be strong evidence that measures' use will lead to better care and outcomes.
- Measures should be used in programs only if they reveal meaningful differences in performance across providers, although some may be retained or reintroduced to reaffirm their importance and verify their continued high level of importance.
- The measures should be administratively simple to collect and report and to the greatest extent possible be derived from electronic health record data.
- Measures should be used to align the efforts of hospitals, physicians and others along the care continuum, and align with the data collection efforts of the other providers.
- Measures should align across public and private payers to reduce unnecessary data collection and reporting efforts.
- Risk adjustment must be rigorous and account for all factors beyond the control of providers, including socioeconomic factors where appropriate. In addition, adjustment methodologies should be published and fully transparent.
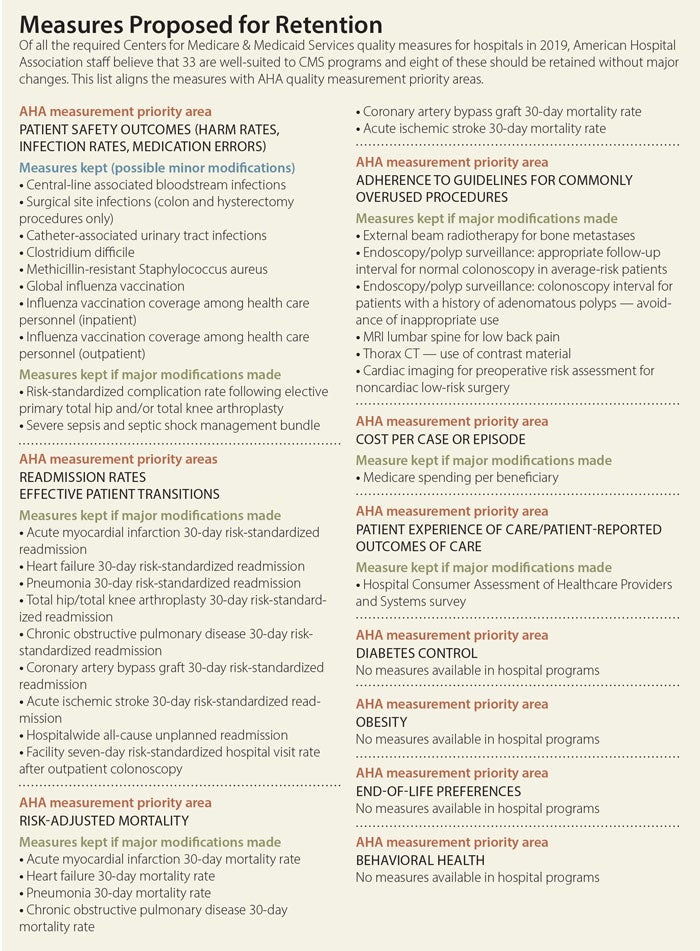
Identifying the CMS measures that best fit the priorities and principles: To provide a “proof of concept” of how the 11 priorities and the measure-selection principles might be applied, AHA staff reviewed the 94 measures that will be required of hospitals in the fiscal year 201 9 Hospital IQR and pay-for-performance programs and the calendar year 2019 Hospital OQR Program. The measures were then placed into three groups: (1) measures that should be retained as is (or with minor changes), (2) measures that require significant modifications to be retained in programs and (3) measures that should be removed. (Given recent CMS rulemaking activity, AHA staff intend to update this analysis in November once the Outpatient Prospective Payment System rule is finalized. Staff do not anticipate the proportions of measures in each category, i.e., retain, modify or remove, will change substantially.)
9 Hospital IQR and pay-for-performance programs and the calendar year 2019 Hospital OQR Program. The measures were then placed into three groups: (1) measures that should be retained as is (or with minor changes), (2) measures that require significant modifications to be retained in programs and (3) measures that should be removed. (Given recent CMS rulemaking activity, AHA staff intend to update this analysis in November once the Outpatient Prospective Payment System rule is finalized. Staff do not anticipate the proportions of measures in each category, i.e., retain, modify or remove, will change substantially.)
AHA staff believe that of the 94 measures reviewed, only 33 are well-suited to CMS programs, and only eight should be retained without major changes. The remaining 61 measures likely should be phased out of CMS hospital measurement programs. When the remaining measures are aligned with the AHA priority areas, it is clear that there are significant gaps in available measures to support quality improvement in critical areas (e.g., diabetes control and obesity). There is significant work to be done to develop or identify relevant measures for some priority areas.
Engaging and convening stakeholders to gain consensus: AHA staff have continually used the 11 AHA priority measure topics to evaluate and respond to proposals for new measures from CMS, the Measure Applications Partnership and others. We intend to continue using the priority areas, along with the measure selection principles, to further engage CMS, MAP and other entities — including private payers — that are measuring hospitals.
For good measure
The AHA also will continue to work with federal agencies, Congress and other stakeholders to help align quality reporting to improve health and health care. This includes improving the fairness of readmission penalties and reforming the HACRP.
Improving the fairness of readmission penalties: The AHA strongly urges CMS to incorporate socioeconomic adjustment into the HRRP so that hospitals caring for our nation’s most vulnerable patients are not unfairly penalized. We strongly support the bipartisan, bicameral Establishing Beneficiary Equity in the Hospital Readmission Program Act of 2015 (HR 1343/S 688). A version of this bill passed the House in June.
Since the HRRP’s beginning, hospitals caring for the poorest patients have been significantly more likely to receive penalties than others have. In fiscal year 2017, nearly 86 percent of hospitals in the highest quartile of disproportionate patient percentage received a penalty, compared with 60 percent in the lowest DPP quartile (higher DPP quartiles indicate a poorer patient population). This is because the HRRP fails to recognize that community factors outside the control of the hospital — such as the availability of primary care, mental health services, physical therapy, easy access to medications and appropriate food, and other rehabilitative services — significantly influence the likelihood of a patient’s health improving after discharge from the hospital or whether a readmission may be necessary.
These community issues are reflected in readily available data on socioeconomic status, such as census-derived data on income and education level, and claims-derived data on the proportion of patients dually eligible for Medicare and Medicaid. If HR 1343/S 688 is passed, CMS would be required to use these data to adjust penalties, providing important relief.
The AHA also urges CMS to exclude from the HRRP readmissions unrelated to the initial reason for admission. Despite the fact that the ACA requires CMS to exclude unrelated readmissions, CMS has not fully implemented this policy. For example, a patient may be hospitalized for pneumonia and then readmitted within 30 days for a hip fracture, which is clearly unrelated to the pneumonia. The current measures would count this readmission against the hospital.
Reforming the HACRP: America’s hospitals are deeply committed to reducing preventable patient harm. However, the HACRP is poorly designed and imposes arbitrary, excessive penalties that disproportionately affect hospitals that tend to care for the sickest patients. The AHA will work with CMS, Congress and others to improve existing policy and promote alternatives to the HACRP that more effectively promote patient safety.
The HACRP has a number of critical flaws. First, the program’s arbitrary design penalizes 25 percent of all hospitals each year, regardless of significant performance improvement, and does not measure meaningful differences in quality. Indeed, the difference in HAC scores for penalized and nonpenalized hospitals in fiscal year 2015 is only hundredths of a point.
Second, data show that hospitals treating patients with complex conditions are disproportionally penalized, in part because the HACRP uses claims-based patient safety indicators that are unreliable and do not reflect important details of a patient’s risk factors and course of care. We have urged CMS to gradually remove PSIs from the HACRP. Third, some small hospitals have too few patients to have data on the two infection measures used in this program. These hospitals are assessed only on the unreliable PSIs.
Finally, the HACRP measures overlap with the measures in the Hospital VBP Program, yet each program uses different performance periods. This can lead to excessive payment penalties and confusion about the true state of hospital performance. To provide short-term relief, the AHA recommends that CMS use measures in either the VBP or the HAC program but not in both.
Akin Demehin (ademehin@aha.org) is director of policy at the American Hospital Association.