
The Ins and Outs of Physician Payment After Medicare Sustainable Growth Rate Reform
On April 16, President Barack Obama signed into law the Medicare Access and CHIP Reauthorization Act of 2015. This historic bipartisan, bicameral legislation repealed the flawed Medicare physician sustainable growth rate formula after 18 years and 17 temporary “patches.” Among its key provisions, the legislation retrospectively halted a 21 percent cut to Medicare physician payments that took effect April 1 and in its place provides predictable payment updates for physicians under the Medicare physician fee schedule.
Even more significantly, the law creates a new physician payment and performance measurement system that ties an increasing percentage of physician payment to value and encourages physician participation in alternative payment models. APMs move payment away from fee-for-service reimbursement and instead pay providers based on the quality and cost of care for particular episodes (e.g., bundled payment) or defined patient populations (e.g., accountable care organizations).
By increasing physician participation in APMs, the Medicare program seeks to move the field away from a fee-for-service model and closer to a payment system tied to patient outcomes and population health. Beginning in 2019, physicians will have two payment “tracks” to choose from for Medicare payment — the Merit-based Incentive Payment System or an APM.
The implementation of the law will have a significant impact not only on physicians but also on the hospitals with which they partner. Indeed, according to the American Hospital Association’s Annual Survey, hospitals employed nearly 245,000 physicians in 2013 and had individual or group contractual arrangements with at least 296,000 more.
Hospitals that employ physicians directly will bear the cost of implementing and complying with the new physician performance reporting requirements as well as face risk for any payment adjustments. Moreover, hospitals may be called upon to participate in alternative payment models so their physician partners can qualify for the APM track.
This executive briefing summarizes key aspects of this new physician payment system. More information is available at www.aha.org/MACRA.
Payment for Value
Beginning in 2019, the new law sunsets three current-law reporting and pay-for-performance programs: the physician quality reporting system, the Medicare electronic health record incentive programs for eligible professionals (also known as meaningful use of the electronic health record) and the value-based payment modifier. These programs will be consolidated into a new MIPS. The MIPS will be the default payment system for physicians, physician assistants, nurse practitioners, clinical nurse specialists and certified registered nurse anesthetists as well as practice groups that include these professionals.
In 2021, the Centers for Medicare & Medicaid Services may expand the program to include other nonphysician professionals who bill under the physician fee schedule, such as therapy providers. Physicians and other professionals who receive a significant portion of their payments through APMs will be exempt from the MIPS and most electronic health record meaningful use requirements.
Physicians will be assessed under four performance categories:
- Quality: CMS may use measures in the current-law programs as well as other measures solicited and approved by the secretary of Health and Human Services.
- Resource use: This category includes the cost measures under the value-based payment modifier program, plus other measures.
- Clinical practice improvement activities: This category is intended to reflect participation in activities such as expanded practice access, population health management, care coordination, Medicare beneficiary engagement, patient safety and practice assessment and participation in an APM. Physicians will receive enhanced ratings under this category for participation in a medical home, a comparable specialty practice or an APM.
- Meaningful use of certified electronic health record technology: This incorporates current-law meaningful use requirements.
The four performance categories will be weighted to determine a total composite score of 0 to 100 points. CMS has flexibility to vary the percentage weights based on factors such as high electronic health record meaningful use adoption and lack of sufficient availability of appropriate measures and activities. Physicians who do not satisfactorily report required data in a particular category will be penalized by receiving the lowest possible score in that category.
CMS must adjust individual measures and/or scoring methodology based on an individual patient’s health status and other risk factors. After the first year, the assessment methodology must take into account the physician’s improvement in the quality and resource use categories and may account for improvement in the other two categories.
Each year, CMS will establish a performance threshold. Physicians’ composite scores will be compared with the performance threshold to determine a payment adjustment factor:
- Physicians at or above the threshold will receive a 0 percent or a positive payment adjustment.
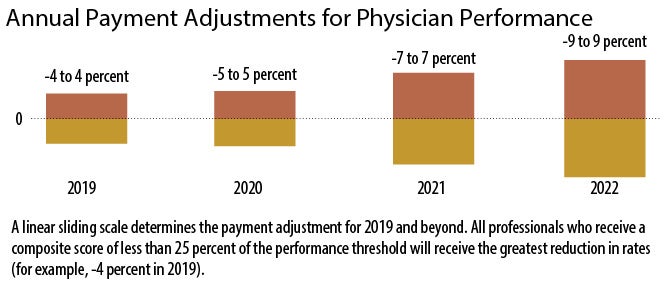
- Physicians below the performance threshold will receive a negative payment adjustment, with lower scores receiving greater negative adjustments. Physicians whose score is one-fourth or less of the threshold will receive the lowest possible adjustment.
The payment adjustment will be determined using a linear sliding scale based on a percentage set in statute for each year — a composite score of 100 would correspond to an adjustment of the highest applicable percentage, while a score of 0 would correspond to an adjustment of the lowest applicable percentage. See the resulting sliding-scale payment adjustments in “Annual Payment Adjustments for Physician Performance” below.
The payment system is budget-neutral. That is, CMS will not be able to pay out more in incentives than it withholds in penalties.
For 2019 through 2024, the HHS secretary will set a threshold for exceptional performance, which may result in an additional payment increase of up to 10 percent. The total aggregate increase in payments resulting from the exceptional performance bonus will be $500 million each year.
New Payment Models
The law creates incentives for physicians to use alternative payment models by developing a separate payment “track” for physicians who receive a significant portion of their payments through APMs. Qualifying physicians will be exempt from the Merit-based Incentive Payment System, including most of its quality reporting provisions, and will receive a bonus of 5 percent of their Medicare physician fee schedule payments annually from 2019 through 2024.
To determine whether a physician sufficiently participates in APMs to earn the bonus payment and MIPS exemption, CMS will consider the percentage of the physician’s payments attributable to services provided through an eligible APM. To encourage increased participation, the percentage required to qualify goes up over time.
In keeping with an emphasis on value, the law targets payment models that meet certain criteria. Specifically, the payment model must require the use of certified electronic health record technology and provide for payment based on quality measures comparable to those used in the MIPS quality category.
Additionally, the entity participating in the APM (and through which the physician provides services) either must be a medical home or must bear financial risk for more than a nominal loss. Eligible APMs under Medicare will include models tested by the Center for Medicare and Medicaid Innovation, a Medicare Shared Savings Program accountable care organization and certain demonstrations under federal law.
Implications for Hospitals
The physician response to the incentives inherent in the new payment system may have both direct and indirect effects on hospitals and health systems. Those that employ physicians likely will bear the implementation and ongoing compliance costs associated with the new physician performance reporting requirements as well as any payment adjustments due to poor performance under the MIPS. In addition, as a greater percentage of physician payments become at risk, an increasing number of physicians may seek stability through hospital employment or contractual relationships.
Finally — so their physicians can be exempt from MIPS participation — hospitals may experience increased pressure to participate in APMs that involve two-sided risk. This may be particularly true with respect to hospital-based specialists, such as hospitalists, whose participation in an APM would be difficult if the hospital didn’t take part.
AHA Resources
The AHA is working with members to identify the most important policy and operational implications of the MIPS and APMs for hospitals. We are educating hospital and physician leaders by providing advisories, webinars and other resources at www.aha.org/MACRA.
Akin Demehin, M.P.H. (ademehin@aha.org), and Melissa Jackson, J.D., M.P.A. (mjackson@aha.org), are both senior associate directors for policy at the American Hospital Association in Washington, D.C.
Predictable Payment Updates
The Medicare Access and CHIP Reauthorization Act provided a 0 percent update from April through June 2015, a 0.5 percent update from July 2015 through 2019 and a 0 percent update from 2020 through 2025 to base rates for physicians and other health care professionals paid under the physician fee schedule. Beginning in 2026, physicians will receive different annual updates depending on whether they are paid under the new Merit-based Incentive Payment System (0.25 percent) or primarily through alternative payment models (0.75 percent update).
Questions for Board Discussion
The Centers for Medicare & Medicaid Services will need to fill in significant details of the new payment system over the coming months and years. In the meantime, hospital board of trustees members and executive leaders may prepare for implementation of the new system by considering the following issues:
- What is the organization’s current level of integration with physicians? Should the organization move toward greater integration, such as through increased physician employment or the formation of a clinically integrated network?
- Will the organization assist physicians with required reporting? If so, will additional infrastructure be required?
- How can the organization best align measures and incentives among facilities and practitioners across the organization?
- Should the organization participate in alternative payment models and, if so, should the organization lead those efforts or partner with others?
— Akin Demehin and Melissa Jackson